- The motor in psychoMOTOR is related to actual motors, cars..
Yes…tragic but true I’ve been asked this so many times. Motor in psychomotor is related to motor skills in bodily functions.
- We play with kids:
I’ve heard this probably each time I’ve told someone that I’m a psychomotor therapist. I’ve had to explain every single time that we target our objectives through “activities” that may be games.
- We only work with kids:
No…not really. Our age frame extends from the premature or born-on-time newborn, to babies, kids, teenagers, adults and elderly people. (What is psychomotor therapy?)
- We only work at private clinics:
Psychomotor therapists can work in hospitals, schools, institutions, NGOs, centers and clinics.
- We read people’s personality through their body language:
We are not mind readers nor psychics. We do not analyze nor comprehend someone through any of their action (and most importantly we have not been taught to do that). In fact, we are not psychologists and therefore are not able and are not entitled to analyze someone’s personality.
- We only target handwriting skills:
No, our main objective is not writing skills. In the context of schools, it might be an important area to work on, but mostly, we target all psychomotor domains (What happens during a session?)
- We analyze a person through their handwriting or their pencil grip:
We might work on our patient’s handwriting but that does not make us experts in understanding him/her, the way he/she thinks. Holding the pencil one way or writing in another may have some meaning but again it is not our job to do that.
- The fact that we face people and kids with difficulties or disorders causes us to become depressed:
No, when you’ve been taught ways to face those situations, to be empathetic and not sympathetic and to practice relaxation (actual methods of relaxation through breathing and mobilizations among other methods and techniques), facing difficult situations and cases will not cause you sadness or depression.
- We are called doctors:
Just cause we might work at hospitals or centers and we might wear scrubs, that doesn’t make us doctors. Through our curriculum, we do take medicine courses (physiology, psychiatry etc.) but that does not make us doctors (unfortunately!).
- We are miracle doers and our patients will all recover:
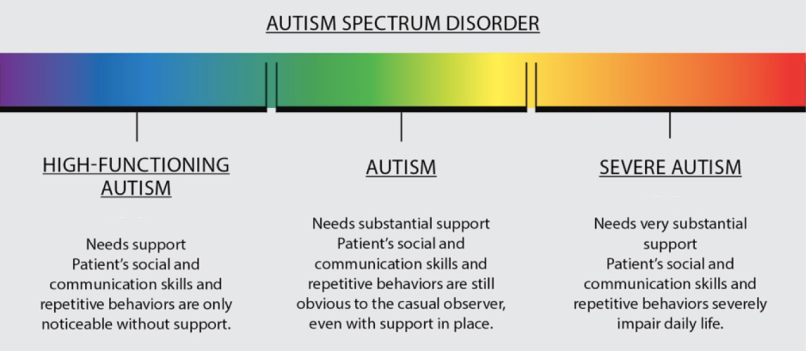
This is probably every therapist and doctor’s dream. We all want all of our patients to recover and “heal” but in so many cases (genetic or neurodevelopmental ones such as down syndrome and autism), people may learn and acquire strategies to live with their difficulties but will never stop having those syndromes. We really wish our job could do that!


 Actual testimonials of people with ASD*:
"I do not like to feel the skin of others, which is either very dry or moist and I will wash my hands regularly as soon as I can."
"When my mother rubbed my hair, my scalp ached ... I also liked wearing long pants, because I hated my legs touching each other. (Grandin, 1996)
"I was very sensitive to food texture and had to first touch them with my hands before putting them in my mouth. "
"When I got home, I noticed that my face was squinted, bleeding through a thousand small cuts. Indeed, he had rubbed me with snow full of small gravel, but I had not felt because of my high pain threshold. "
Actual testimonials of people with ASD*:
"I do not like to feel the skin of others, which is either very dry or moist and I will wash my hands regularly as soon as I can."
"When my mother rubbed my hair, my scalp ached ... I also liked wearing long pants, because I hated my legs touching each other. (Grandin, 1996)
"I was very sensitive to food texture and had to first touch them with my hands before putting them in my mouth. "
"When I got home, I noticed that my face was squinted, bleeding through a thousand small cuts. Indeed, he had rubbed me with snow full of small gravel, but I had not felt because of my high pain threshold. "